

Quick Numbers
| Norwood stages | 7 stages (1–7), with sub-stages 2A, 3A, 3V, 4A, 5A |
|---|---|
| Medication trial period | 12–18 months before assessing response |
| Typical surgery threshold | Norwood 3V and above, or medication non-responders |
| Graft survival (surgeon-led FUE) | Up to 98% |
| Multi-session interval (Norwood 4+) | Minimum 6 months between sessions |
Key Takeaways
| Finasteride and minoxidil can stabilize or partially reverse Norwood 2–3 loss, but they rarely regrow hair in bald Norwood 5+ zones. |
| A 12- to 18-month medication trial helps separate responders from non-responders before committing to surgery. |
| Norwood 4 and higher typically requires at least two surgical sessions spaced six months apart to protect the donor area. |
| Combining post-operative medication with surgery produces the best long-term density because it slows native hair loss behind the transplanted zone. |
| Surgical planning is among the most critical steps: hairline position, graft budget, and donor preservation all depend on accurate Norwood staging. |
A 32-year-old man notices his temples have crept back about two centimeters over three years. His dermatologist prescribed finasteride eight months ago, and the shedding slowed, but the frontal recession hasn't reversed. He's now asking the question that roughly 50 million men in the United States alone eventually face: at what point does male pattern baldness stop responding to medication, and when does surgery become the rational next step? The answer isn't a single Norwood number or a calendar date. It's a clinical decision that weighs staging, medication response, donor supply, age, and realistic expectations.
What Is the Norwood Scale and Why Does Staging Matter?
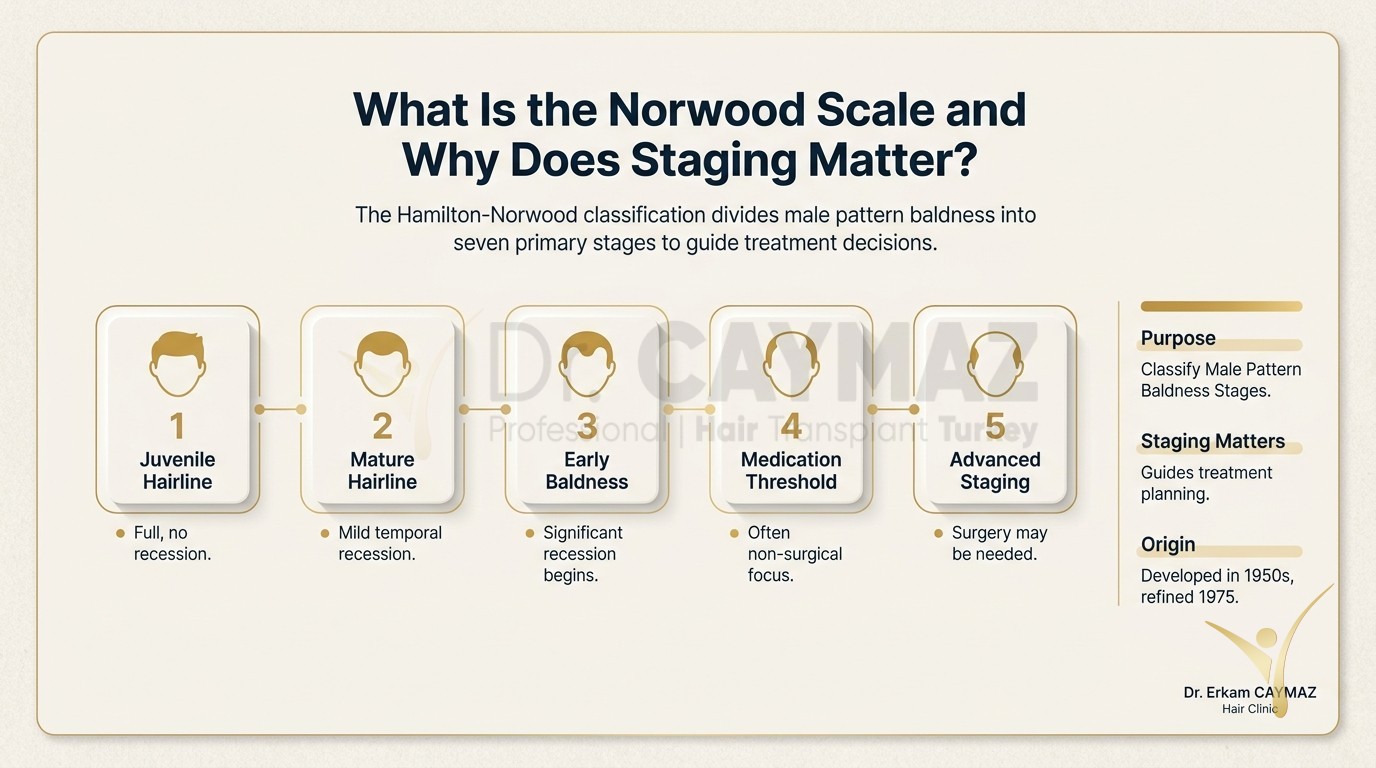
The Hamilton-Norwood classification, first published in the 1950s and refined in 1975, divides male pattern baldness into seven primary stages. Stage 1 is a full juvenile hairline with no recession. Stage 2 shows mild temporal recession, often called "mature hairline" rather than true baldness. By stage 3, the temples have receded enough to form an M-shape, and the variant 3V adds early vertex (crown) thinning. Stages 4 through 7 describe progressively larger bald areas on the frontal scalp and crown, until stage 7 leaves only a horseshoe-shaped fringe of donor hair around the sides and back.
Staging matters because it predicts two things: how much area needs coverage and how much more loss is likely coming. A 25-year-old at Norwood 3 with a strong family history of Norwood 6 faces a very different planning equation than a 45-year-old at Norwood 3 whose loss has been stable for a decade. Understanding how the hair loss process unfolds over time helps patients set realistic timelines for both medication and surgery.
One common mistake is treating the Norwood scale as a simple countdown. Not every man progresses through every stage. Some stabilize at Norwood 3 for decades. Others sprint from 3 to 5 in under five years. Genetic predisposition, androgen sensitivity, and age of onset all influence the speed. That's exactly why a medication trial before surgery isn't wasted time: it reveals your personal rate of progression.
How Do Finasteride and Minoxidil Work Against DHT-Driven Loss?
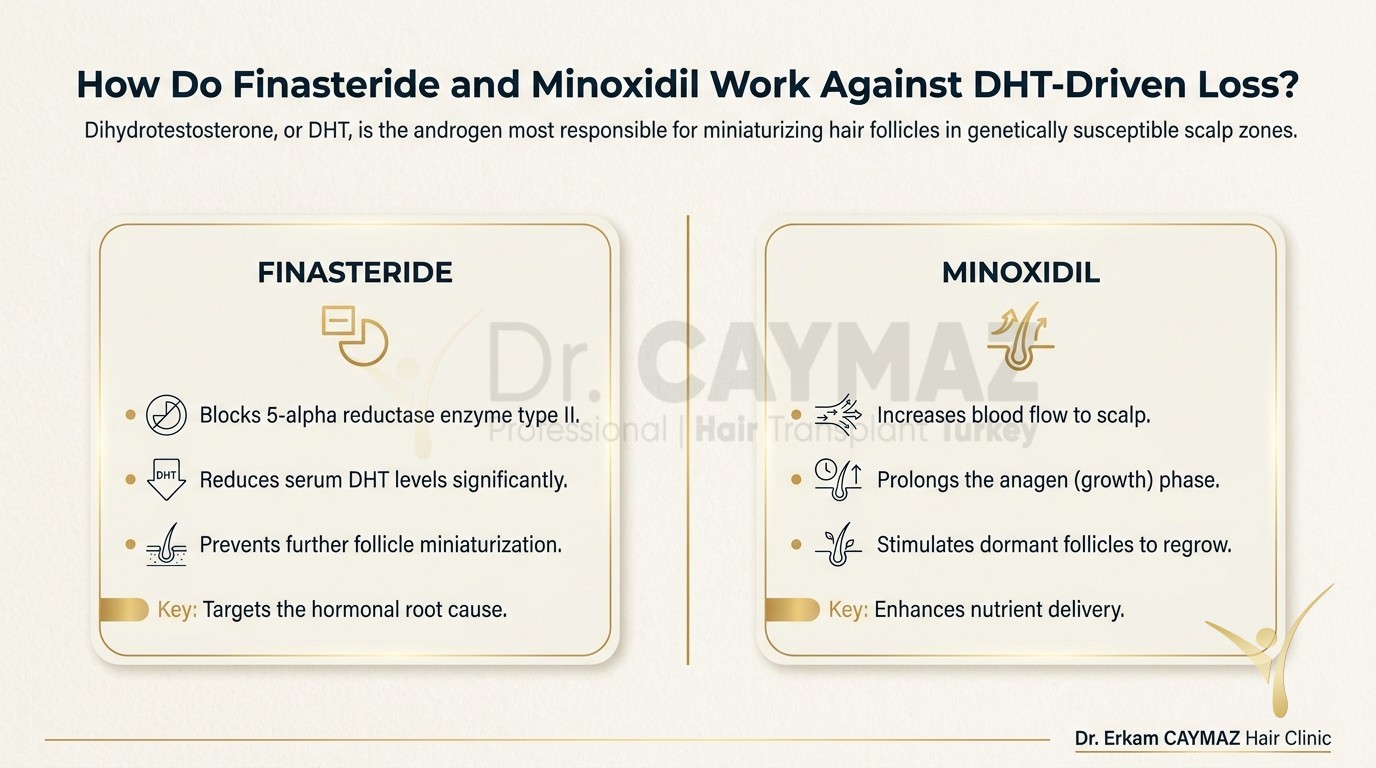
Dihydrotestosterone, or DHT, is the androgen most responsible for miniaturizing hair follicles in genetically susceptible scalp zones. Testosterone converts to DHT via the enzyme 5-alpha reductase. Finasteride blocks the type II isoform of that enzyme, reducing serum DHT levels by roughly 70%. Dutasteride blocks both type I and type II isoforms and can lower DHT by over 90%, though it's prescribed off-label for hair loss in most countries.
Minoxidil, applied topically at 5% concentration, works through a different mechanism. It's a vasodilator that prolongs the anagen (growth) phase of the hair cycle and may stimulate follicular potassium channels. It doesn't block DHT. The two medications are often used together because they target different pathways. You can read a detailed breakdown of finasteride and minoxidil dosing, side effects, and expected results for clinical specifics.
Here's the clinical reality: these medications work best on miniaturizing follicles, meaning hairs that are thinning but not yet dead. In Norwood 2 and early Norwood 3, a significant percentage of frontal and mid-scalp follicles are still miniaturizing rather than fully dormant. That's the window where medication can stabilize loss and sometimes produce visible regrowth. Once a follicle has been dormant for several years and the follicular unit has fibrosed, no oral or topical medication currently available can resurrect it.
When Should You Consider Medication Alone Sufficient?
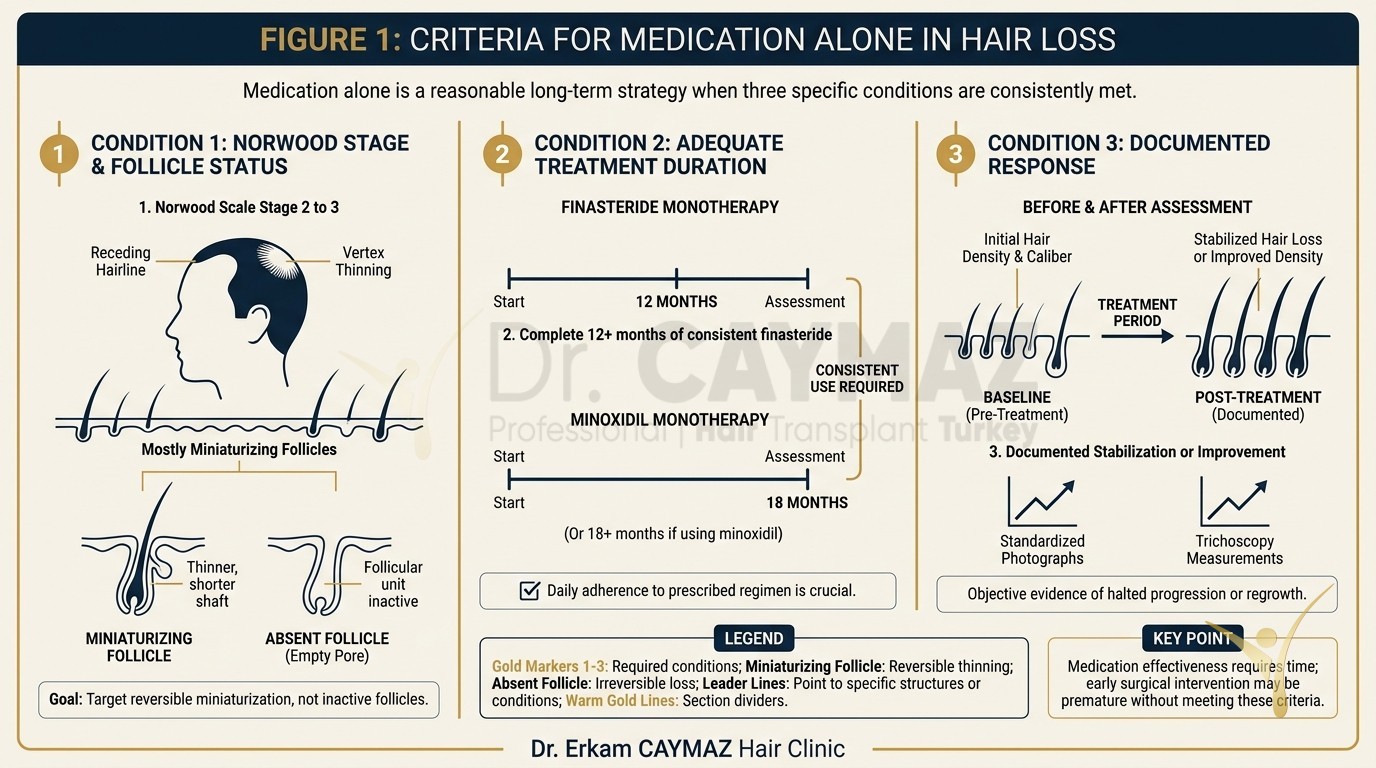
Medication alone is a reasonable long-term strategy when three conditions are met. First, you're at Norwood 2 to 3 with mostly miniaturizing rather than absent follicles. Second, you've completed at least 12 months of consistent finasteride use (or 18 months if using minoxidil monotherapy) and documented stabilization or improvement through standardized photos. Third, you're comfortable with the cosmetic result that medication provides, even if it doesn't restore a juvenile hairline.
Patients who respond well to finasteride within the first year often maintain that response for five to ten years, according to long-term extension studies. The key word is "maintain." Medication typically holds the line rather than pushing it forward dramatically. If you're 28, at Norwood 2A, and your photos show no further recession after 14 months on finasteride, surgery may genuinely be unnecessary for years.
PRP (platelet-rich plasma) injections can serve as an adjunct during this medication-only phase. They don't replace finasteride or minoxidil, but some clinical data suggests PRP can improve hair caliber in early-stage thinning. Our clinic offers PRP treatment for hair loss as a supportive therapy, not a standalone cure.
What Are the Signs That Medication Has Reached Its Limit?
Several clinical signals indicate that you've crossed the threshold where medication alone won't deliver the density you want.
Continued recession despite compliance. If you've taken finasteride daily for 18 months and your temples are still receding in serial photographs, you're a partial or non-responder. Roughly 15–20% of men fall into this category. Switching to dutasteride may help some, but the gains are incremental, not dramatic.
Visible scalp through the forelock. When the mid-scalp behind your hairline thins enough that scalp skin is visible under normal lighting, you've lost enough density that medication alone can't restore the optical illusion of fullness. This typically corresponds to Norwood 3V or early Norwood 4.
Crown expansion beyond a 5 cm diameter. Vertex thinning that has spread to a circle wider than about 5 centimeters rarely fills back in with topical minoxidil alone. The crown is notoriously medication-resistant once the bald patch is established, because the follicles in the center have often been dormant the longest.
Age and stability plateau. A man in his late 30s or 40s whose loss has been stable at Norwood 3–4 for three or more years is actually an excellent surgical candidate. His pattern is predictable, his donor area is assessable, and the risk of rapid future loss undermining the transplant result is lower. Understanding whether medication or transplant should come first depends heavily on this stability assessment.
Dr. Caymaz Insight
| I tell every patient under 30 at Norwood 2–3 the same thing: give finasteride a full 12 to 18 months before we discuss surgery. That trial period isn't a delay, it's diagnostic. It shows me your rate of loss, your medication response, and how much native hair we can preserve behind whatever grafts I place. When I design a hairline, I'm planning for the next 20 years of your face, not just today's recession. Rushing to surgery before we understand your loss trajectory is one of the most common planning errors I see in revision cases from other clinics. |
How Does Norwood Stage Affect the Surgical Plan?
Surgical planning for male pattern baldness goes beyond counting grafts. It's about distributing a finite donor supply across current and anticipated future loss zones. The average male donor area contains between 5,000 and 7,000 extractable grafts over a lifetime, depending on density, scalp laxity, and hair caliber. That's a budget, and every Norwood stage spends it differently.
| Norwood Stage | Estimated Graft Need | Sessions Recommended | Primary Strategy |
|---|---|---|---|
| 2–2A | 800–1,500 | 1 | Medication first; surgery if non-responder after 12–18 months |
| 3–3V | 1,500–2,500 | 1 | Surgery reasonable if loss is stable; continue medication post-op |
| 4–4A | 2,500–3,500 | At least 2 | Session 1: frontal zone. Session 2: crown, minimum 6 months later |
| 5–5A | 3,500–5,000 | 2–3 | Prioritize frontal third; crown coverage depends on donor reserves |
| 6–7 | 5,000–7,000+ | 2–3 | Frame the face first; full crown coverage may not be achievable |
For patients at Norwood 4 and above, Dr. Caymaz recommends at least two sessions spaced a minimum of six months apart. This protects the donor area from overharvesting, a problem that can leave permanent visible thinning at the back of the scalp. Single-session mega-procedures of 5,000 or 6,000 grafts carry real risks of donor depletion and poor graft survival due to extended out-of-body time. You can see why large graft counts require multiple sessions in our clinical breakdown.
The technique choice also shifts with staging. Sapphire FUE is the default standard for most cases because the sapphire-tipped blades create smaller, more precise recipient channels that heal with minimal scarring. For patients who need density packing into existing hair without shaving,
DHI with Choi implanters can be appropriate in select zones. The decision between techniques depends on the recipient area's characteristics, not marketing preference.
Why Is Hairline Design the Most Critical Variable at Every Stage?
A hairline placed too low at Norwood 3 will look unnatural by the time the patient reaches Norwood 5, because the transplanted line will sit on an island of density surrounded by thinning native hair. A hairline placed too high wastes the patient's current density and makes him look older than necessary. The sweet spot requires predicting future loss, which is why surgical planning is among the most critical steps in the entire process.
At our clinic, Dr. Erkam Caymaz personally handles every hairline design and performs the VIP incisions that define angle, depth, and direction of each recipient channel. This step, called The Architect Touch, determines whether the final result looks natural or artificial. Extraction and implantation are carried out by expert surgical technicians under his direct supervision, while he focuses on the design and incision architecture that shape the aesthetic outcome.
For Norwood 3 patients, the hairline typically sits at the upper border of the frontalis muscle contraction, roughly 7 to 9 centimeters above the glabella (the bony ridge between the eyebrows). For Norwood 5 and above, the hairline may be set slightly higher to ensure adequate density across a larger area. Single-hair grafts are placed along the very front edge to mimic the natural feathered transition, while multi-hair grafts build density behind that leading row.
What Happens After Surgery: Do You Still Need Medication?
Transplanted grafts are harvested from the DHT-resistant donor zone at the back and sides of the scalp. These follicles retain their genetic resistance to miniaturization even after relocation, which is why a hair transplant is considered permanent. However, the native hairs surrounding the transplanted grafts are not immune. Without ongoing medication, those native hairs can continue to thin, creating an unnatural contrast between dense transplanted zones and thinning native zones over time.
This is why most surgeons, including our team, recommend continuing finasteride (or dutasteride) after surgery for patients whose loss is still progressing. The medication protects the investment by preserving native density around the grafts. You can read about post-transplant finasteride protocols for specific dosing guidance.
Post-operative care also affects graft survival. The first two weeks are the most critical window. At our clinic, the first wash and donor bandage removal occur on day 2 post-op, following a full rest day after surgery. For example, a Monday operation means Tuesday rest, Wednesday first clinic wash. This timing allows initial fibrin clot stabilization before gentle cleansing begins. Detailed aftercare protocols cover everything from sleeping position to sun exposure during the healing weeks.
Medication-Surgery Combination: The Strongest Long-Term Outcome?
The clinical evidence consistently shows that the best long-term results come from combining surgical restoration with ongoing medical therapy. Surgery restores density in areas where follicles are gone. Medication preserves density in areas where follicles are miniaturizing but still alive. Neither approach alone covers both needs.
Consider a Norwood 4 patient who receives 3,000 grafts to rebuild his frontal zone and mid-scalp. If he stops finasteride after surgery, his crown and the transition zone behind the transplanted area may continue thinning over the next five to seven years. By year seven, he could look like he has a dense island of hair in front and a thinning halo behind it. That's not a surgical failure; it's a medication compliance failure.
For patients who can't tolerate oral finasteride due to side effects, topical finasteride formulations (typically 0.1% to 0.25%) offer a lower systemic exposure alternative. Low-level laser therapy and mesotherapy can serve as additional supportive measures, though neither replaces anti-androgen therapy for DHT-driven loss.
The bottom line is straightforward. Medication buys time and preserves native hair. Surgery restores what medication can't. Using both together, calibrated to your Norwood stage and rate of progression, produces the most durable, natural-looking result over a 10- to 20-year horizon.
How Do You Know If You're Ready for a Consultation?
If you've been on finasteride for at least 12 months and your loss has stabilized but your density doesn't satisfy you, you're a reasonable surgical candidate. If you've never tried medication and you're under 30, a medication trial first is almost always the smarter sequence. If you're over 35 with stable Norwood 4+ loss and adequate donor density, surgery is likely the primary intervention, with medication as the supporting player.
A proper consultation should include standardized photographs, donor density measurement (ideally 60+ follicular units per square centimeter for good candidacy), a family history review, and a frank discussion about what's achievable in one session versus two. At
our clinic, we perform only 1 to 2 VIP operations per day, which means every patient receives the surgeon's full attention during planning, design, and incision phases.
Don't let anyone tell you that a single massive session of 5,000+ grafts will solve Norwood 5 in one afternoon. Donor preservation is a non-negotiable principle. The grafts you don't harvest today are the grafts available for a touch-up or second session years from now. Responsible staging of the surgical plan is what separates a result that ages well from one that creates new problems.
Sources
FAQ
Medication is most effective when started early, ideally at Norwood 2 or 3 while follicles are miniaturizing rather than fully dormant. Starting finasteride at this stage can stabilize loss and sometimes produce partial regrowth. The earlier you begin, the more native hair you preserve.
A minimum of 12 to 18 months on finasteride is recommended before evaluating whether you're a responder or non-responder. This trial period provides standardized photo evidence of stabilization or continued loss, which directly informs the surgical plan.
No. Finasteride works on miniaturizing follicles that are still producing thin, short hairs. Once a follicle has been dormant for several years and the follicular unit has fibrosed, no currently available medication can revive it. Surgery is the only option for restoring hair in fully bald zones.
Norwood 4 and higher typically needs 2,500 to 5,000 or more grafts. Extracting that many in a single session risks overharvesting the donor area, which can cause permanent visible thinning at the back of the scalp. Two sessions spaced at least six months apart allow the donor zone to heal and ensure better graft survival.
In most cases, yes. Transplanted grafts are DHT-resistant and permanent, but your native hairs surrounding the transplanted zone can continue to thin. Continuing finasteride after surgery preserves those native hairs and prevents an unnatural density contrast over time.
Overall success rates for FUE hair transplant surgery range from 90 to 95%, with graft survival rates reaching up to 98% in surgeon-led procedures with proper technique and aftercare. No clinic can guarantee 100% results, as individual healing and compliance affect outcomes.

Should I Use Finasteride After Hair Transplantation?
After hair transplantation, patients often ask whether medication is necessary to protect their result. The honest…
Read More
Hair Transplant Surgery in The Summer
Hair transplant can be performed in summer when aftercare rules are followed. The season itself is not the main risk…
Read More
Hair Transplantation and the Effect of Scalp Tissue
Scalp tissue quality influences extraction safety, implantation response, and cosmetic durability. Temporary donor…
Read More
Pubic Hair Transplantation for Female
Pubic hair transplant (PHT) moves scalp follicles to the bikini zone to restore density, shape, or scars after waxing…
Read MoreFrequently Asked Questions
Professional Hair Transplant Insights by Dr. Erkam Caymaz